NUTRITION TO OPTIMIZE RECOVERY AFTER SURGERY

Why does perioperative nutrition matter?
Patients with poor nutritional status prior to surgery are more likely to suffer complications after surgery including infection and death, have a greater hospital length of stay and cost of hospitalization, and are more likely to be readmitted to the hospital within 30 days after surgery.1But it is important to note that malnutrition is one of the few modifiable preoperative risk factors. In fact, nutritional therapy has been shown to improve outcomes in surgeries such as gut or cancer surgery, where there is a greater risk of preoperative malnutrition.
How can nutritional status be assessed before surgery?
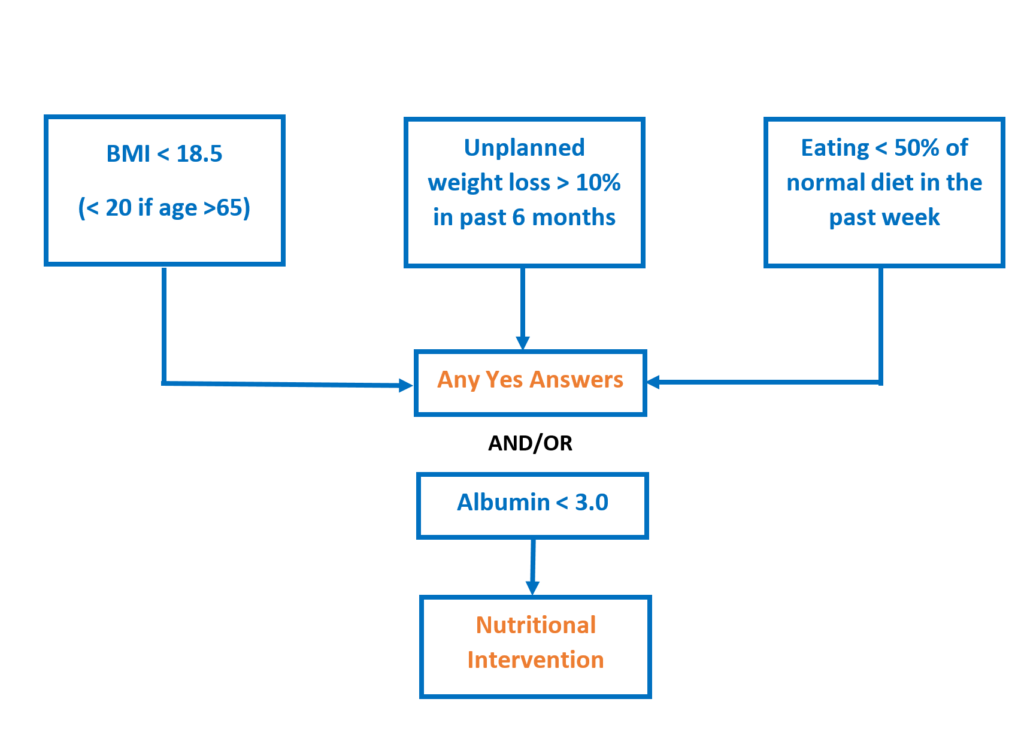
A number of screening tools are available and the perioperative nutrition screen (PONS) is one that is easy to apply in the preoperative period. This tool uses body mass index (BMI – a measure that combines height and weight), recent change in weight, recent decrease in food intake, and preoperative blood albumin level (a rough measure of nutritional state that is commonly tested before surgery). A nutritional intervention is recommended if there are 1 or more positive responses on the PONS.
How does surgery alter nutritional needs?
The surgical stress response results in whole-body catabolism (breakdown of complex molecules to smaller ones). This is seen principally as the wasting of muscle, releasing amino acids to allow the synthesis of proteins known as acute phase reactants and production of glucose needed as an energy source.2 In addition, perioperative fasting can worsen the surgical stress response, weaken gut function, and amplify protein losses. Thus, patients who are malnourished, undernourished or muscle-depleted are particularly vulnerable and need nutritional supplementation.
What can be done to improve perioperative nutrition?
Preoperative – Since protein, requirements are increased by the surgical stress response; current recommendations are that patients should receive at least 1.2-2.0 grams of protein/kilogram of body weight/day.1 Studies show that 25-30 grams of protein in a single meal results in the most protein synthesis and is optimal when repeated multiple times per day.3 Patients who are screened at risk for poor nutritional status should receive a high-protein oral nutritional supplement containing at least 18 grams protein/dose, 2-3 times/day for a minimum of 7-14 days. In addition, in many (but not all) patients and in order to minimize the detrimental effects of fasting, clear fluids can be taken up to 2 hours prior to anesthesia. Similarly, at least 45 grams of a carbohydrate drink as a clear liquid taken 2-3 hours before surgery may, in many surgeries, improves insulin sensitivity (typically decreased by the surgical stress response) and results in better blood sugar control. The addition of specific nutritional elements such as glutamine, hydroxymethylbutyrate, zinc, and bromelain, that can reduce postoperative muscle breakdown, support immune function, optimize gut function, and reduce pain and swelling should also be considered.
Postoperative – For most surgeries, early resumption of oral intake is recommended as tolerated. Once again, protein supplementation is needed during the recovery period to maintain lean muscle mass. This can be accomplished using a high-protein diet (1.5-2.0 grams/kilogram of body weight/day) or oral nutritional supplements. Nutritional supplementation, which again include elements like glutamine, hydroxymethylbutyrate, zinc, and bromelain, should continue for a minimum of 4-8 weeks after surgery and possibly up to 3-6 months after surgery in those who are severely malnourished. It is important to remember that the protein intake goal is more important than total calorie intake during this period of healing and recovery.
- Wischmeyer PE, Carli F, Evans DC, et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Nutrition Screening and Therapy Within a Surgical Enhanced Recovery Pathway. Anesth Analg. 2018;126(6):1883-1895.
- Gillis C, Wischmeyer PE. Pre-operative nutrition and the elective surgical patient: why, how and what? Anaesthesia. 2019;74 Suppl 1:27-35.
- Paddon-Jones D, Campbell WW, Jacques PF, et al. Protein and healthy aging. Am J Clin Nutr. 2015;101(6):1339S-1345S.